
Closed loop control of end tidal anesthetic concentration
GE EtC provides an “autopilot” for end tidal anesthetic gas




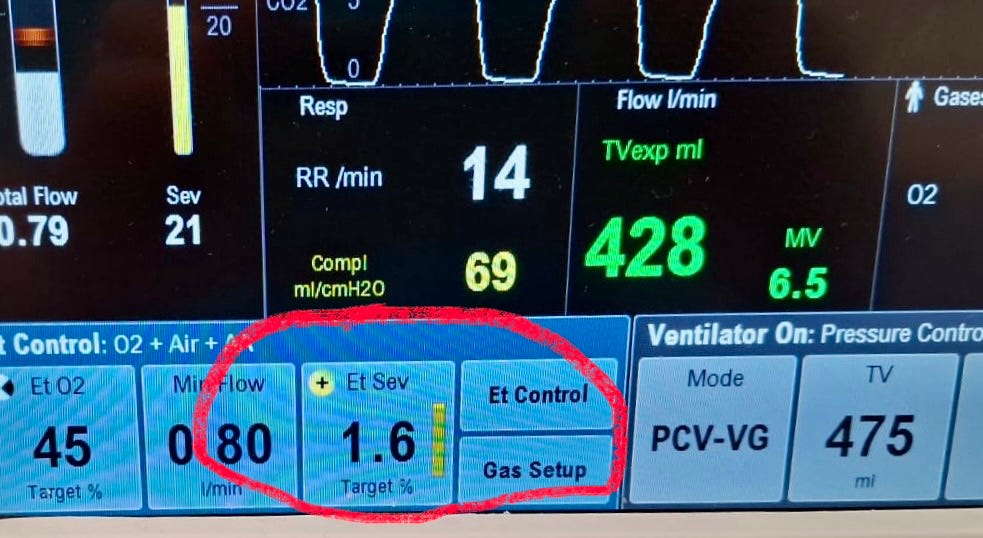
Figure 1. The graphic user interface of a GE anesthesia machine, with closed loop end tidal control of anesthetic agent activated. Photo by Dr. Mark Edwards, taken in Auckland NZ
A closed loop system is an automatic control setup utilizing feedback, where sensors measure the output and compare it with a target, adjusting the input to reduce error. A household thermostat is a common example of closed loop control. The “autopilot” of an aircraft is a very sophisticated and complex example of a closed loop system.
It seems like closed loop systems might be useful in various medical settings, and in fact over the years there have been quite a few experiments with closed loop technology with medical applications. Arguably the most important of these has been closed loop control of type 1 diabetes, in which a closed loop controller interacts with a glucose sensor and an insulin infusion pump to maintain the glucose level within a target range.
The potential applications of closed loop control in anesthesia have been reviewed previously. Examples of application of closed loop systems in anesthesia include the use of computerized electroencephalography, such as BIS, as the output target for anesthetic administration, such as for control of a continuous propofol infusion. Interestingly, Morley et al found no advantage for a closed loop controller using BIS as the target for propofol/alfentanil or isoflurane administration, in comparison to manual control.
Another example of a closed loop system for anesthesia is the use of a twitch monitor as the output for the input of an infusion of a neuromuscular blocker, which has been reported repeatedly since the 1980s.
Janda et al reported successful use of a closed loop system to administer both propofol and mivacurium using BIS and twitch height measured by EMG as the target outputs.
Not all systems that involve computerized control of drug administration are closed loop. In particular, Target Controlled Infusion (TCI—also known as Computer Assisted Continuous Infusion—CACI) utilizes a smart pump and pharmacokinetic models to attempt to attain a target plasma concentration of a drug. But the actual concentration is not measured, so there is no performance feedback to the controller—it’s open loop, not closed loop.
It is important to note, that none of the closed loop systems for anesthesia described above has ever been commercially available or routinely used!
That is, until GE incorporated closed loop control of end tidal anesthetic and O2 concentrations into its anesthesia machines (Figure 1)!

Figure 2. GE electronically controlled vaporizers facilitate closed loop end tidal anesthetic gas control.
GE refers to its system as “EtC” and it is described in an article in Anesthesia and Analgesia published in 2024. Although this system was introduced in Europe in 2010, it was not approved by the FDA for use in the United States until 2022. We do not have GE anesthesia machines at our hospital in Seattle, but our coauthor Mark Edwards has GE machines equipped with EtC in his practice in New Zealand.
Essentially the GE system works by automatically adjusting both the vaporizer and the fresh gas flow to reach the target end-tidal anesthetic and O2 targets set by the anesthesia provider. The system is designed to reach the targets rapidly, but also to minimize fresh gas flow as much as possible to reduce waste of the anesthetic agent.
We highly recommend watching an excellent video presentation by a GE engineer that describes the function of the system.
The GE EtC system is the first example of a commercialized closed loop anesthesia administration system. In our opinion, it’s a game changer. We would not want to surrender our home thermostat for manual control of our furnaces or air conditioners. However, let’s just pause briefly. Just because we are ABLE to use a closed loop system for administration of anesthetics, doesn’t necessarily mean that we WANT to do so. Whether we “can” and whether we “want” are separate questions. If we had EtC we think we would want to use EtC. Mark Edwards has EtC, he uses it regularly, likes it and finds it much more accurate than manual control. The anesthesia providers who used EtC in the clinical trial reported in Anesthesia and Analgesia in 2024 also liked it.
An advantage for closed loop automation is reducing the task burden on providers, freeing them to pay greater attention to solving problems or dealing with unique situations. This is clearly the case for automation in aviation, where autopilots and other automated systems perform many routine tasks, freeing up the attention of pilots to deal with non-routine issues. Zheng and Meister have emphasized the relative slowness of human brain processing and inability to focus attention on more than a single item at a time, which constitutes a powerful argument for automation, especially in complex situations that require simultaneously solving multiple problems or simultaneously completing multiple tasks.
An example of automation in anesthesia that does not involve drug administration, but does free anesthesia providers to pay greater attention to problem solving, is computerized anesthesia record keeping. It’s hard to imagine a pilot of a commercial airliner recording all of the aircraft data by hand, every 5 minutes. Yet that is what all anesthesia providers did for years, and some still do.
Will the GE system be the first of more closed loop anesthesia systems to come in the future? We predict that we will see a commercially available closed loop system for administering neuromuscular blocking drugs by continuous infusion, combined with electromyographic (EMG) twitch monitoring. We will set the target twitch, for example, train-of-four count of 1 or post tetanic count of 2, and the system will administer rocuronium to reach and maintain that target. When will we see this? Our crystal ball is a bit cloudy on the exact timing. We will just say, pretty soon. Stay tuned.
 | A guest post by
|
 | A guest post by
|
 | A guest post by
|
Andy: Nice summary. As you point out the Europeans have been in the business of closed loop anesthetic gas delivery for years. I cannot believe it has taken us so long.