


The Myth of Phase 1 and Phase 2 Block From Succinylcholine
There is always fade in the train-of-four ratio during onset and recovery from succinylcholine block

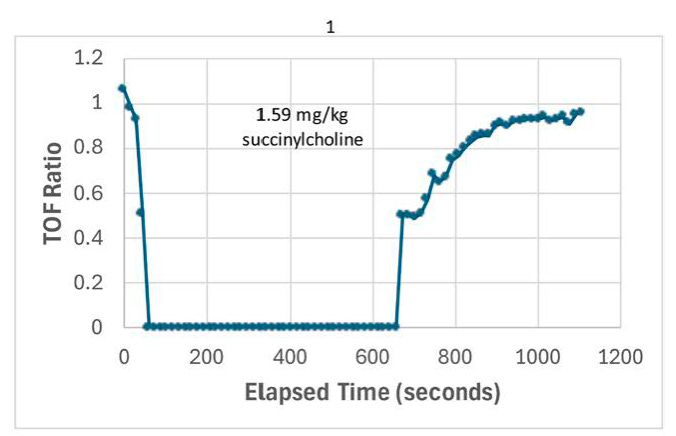
Fade in the train-of-four ratio during onset and recovery from a bolus dose of succinylcholine, from recent article by Michael Todd
Our friend and colleague Michael Todd has just published an outstanding article entitled “The myth of the phase 1 block after succinylcholine in clinical practice”.
Phase 1 block refers to normal depolarizing block with succinylcholine, in which the muscle is depolarized and unresponsive (Figure 2). Traditionally, we have all been taught that during Phase 1 block, there is no fade in the train-of-four ratio. Twitch height is supposedly diminished, but there is supposed to be no fade in the train-of-four, no tetanic fade and no post-tetanic potentiation. Phase 2 block refers to a block that resembles non-depolarizing block, in which the muscle becomes repolarized (following initial, Phase 1 depolarization) but is unresponsive to acetylcholine. This is also referred to as desensitization block. There is fade in the train-of-four ratio, tetanic fade and post-tetanic potentiation. Supposedly Phase 2 block would occur with larger doses of succinylcholine or prolonged administration. Phase 2 block may be antagonized by neostigmine, although perhaps not in every case.
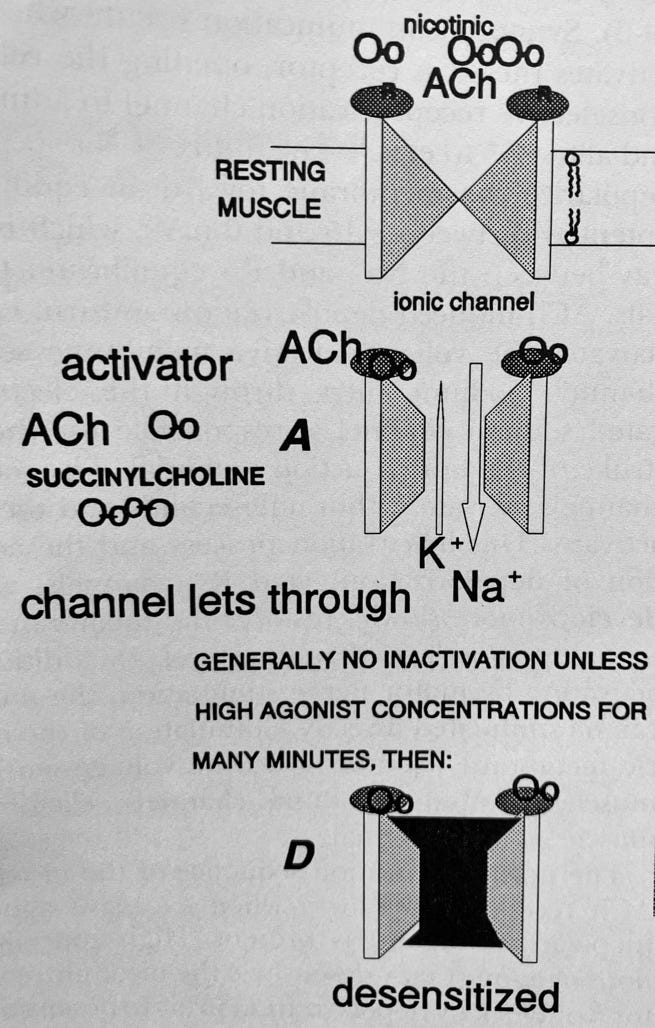
Figure 2. Acetylcholine or succinylcholine activates the nicotinic receptor, producing depolarization of the muscle. Succinylcholine remains on the receptor, producing Phase 1 or depolarization block. If the acetylcholine or succinylcholine remains on the receptor for a period of time, the receptor becomes desensitized and unresponsive even though the muscle becomes repolarized. From Basic Pharmacology of Neuromuscular Blockers by Eugene M. Silinsky in The Pharmacologic Basis of Anesthesiology, Bowdle, Horita and Kharasch editors (1994).
The recently published American Society of Anesthesiology guidelines document on monitoring of neuromuscular blockade states, “Blockade monitoring after succinylcholine reveals a different pattern of recovery than after a nondepolarizing agent, with gradual but equal [NO FADE] return of twitch height as blockade resolves in patients with normal pseudocholinesterase activity.”
Despite this entrenched dogma about succinylcholine block, the traditional concept of Phase 1 and Phase 2 block with succinylcholine turns out to be a MYTH. And, there has actually been plenty of evidence that it’s a myth since at least 1967, when de Jong and Freund published a paper demonstrating fade in the train-of-four ratio, tetanic fade and post tetanic potentiation from the ONSET of block induced by continuous infusion of succinylcholine. This was later confirmed by Naguib et al with bolus doses of succinylcholine. Also confirmed by Kim et al.
Michael Todd has shown this yet again, demonstrating that there is fade in the train-of-four ratio during onset and recovery from bolus doses of succinylcholine. Dr. Todd writes, “the observations here are not new but rather appear to have been largely forgotten.”
Can there be any doubt? Not really. I have been observing the twitch response to succinylcholine administered by bolus or continuous infusion (for thoracic surgery bronchoscopy) in 100s of cases since implementing quantitative twitch monitoring in our practice several years ago. I see fade in the train-of-four ratio during onset and recovery from succinylcholine block in every single patient.
Clearly, the presence of fade does not identify so-called Phase 2 block. So does Phase 2 block exist? Probably it does exist. I very occasionally see cases in which there is prolonged block after succinylcholine infusion and have been able to reverse the block with neostigmine. Perhaps this corresponds to what has been called Phase 2 block. A caveat to this is that a deficiency of pseudocholinesterase activity may result in prolonged block after succinylcholine, and this may not be reversible with neostigmine.
Why has the myth of Phase 1 and Phase 2 block with succinylcholine persisted for so long, despite evidence to the contrary? I think the most likely reason for this is that subjective twitch monitoring would actually miss much of the fade associated with succinylcholine. Thus it would be easy to believe that succinylcholine was causing the twitch amplitude to decrease, without producing fade. We know that fade is difficult to detect by palpation when the train-of-four ratio is greater than about 0.4. Now that we are routinely using quantitative twitch monitoring, we are easily able to measure fade that we did not previously appreciate.
Is there clinical importance to the fact that succinylcholine causes fade in the train-of-four ratio? There are some very practical clinical implications. First, it is possible to monitor succinylcholine paralysis with the train-of-four. The American Society of Anesthesiology guidelines document states that “The only way to effectively monitor both normal and abnormal succinylcholine-induced neuromuscular blockade is by measuring a single twitch baseline height and using the percentage of that single twitch to gauge return of strength.” This is clearly not correct. Monitoring the train-of-four ratio works quite well. Second, it is important to realize that fade in the train-of-four occurs whenever succinylcholine is administered and does not by itself identify a prolonged or so-called Phase 2 block.
I now avoid using the terms Phase 1 and Phase 2, as I don’t think we really understand what they mean. I would simply say that sometimes we see prolonged duration of succinylcholine induced block. Sometimes it seems to be due to decreased pseudocholinesterase activity, and sometimes it may be due to so-called Phase 2 block.
It is very interesting that we have been using succinylcholine since 1951, but we still don’t completely understand its pharmacology.
Once upon a time, I was taught that "not all Phase II blocks are long acting, but all long acting blocks are Phase II." There are clearly very prolonged blocks after large or repeated doses of sux - and they clearly show nondepolarizing characteristics (fade). But as noted, SHORT blocks with a single dose of sux - at least doses similar to those we use routinely - always have characteristics of a nondepolarizing block.